OUR RESEARCH.How does chromosomal instability lead to tumour development and other age-associated diseases? Why is aging the biggest risk factor for cancer? How do the stroma, immune cells and exosomes participate in ageing-related disease? How do tumours acquire resistance to chemotherapy?
|
Our lab seeks to answer these fascinating questions and more!
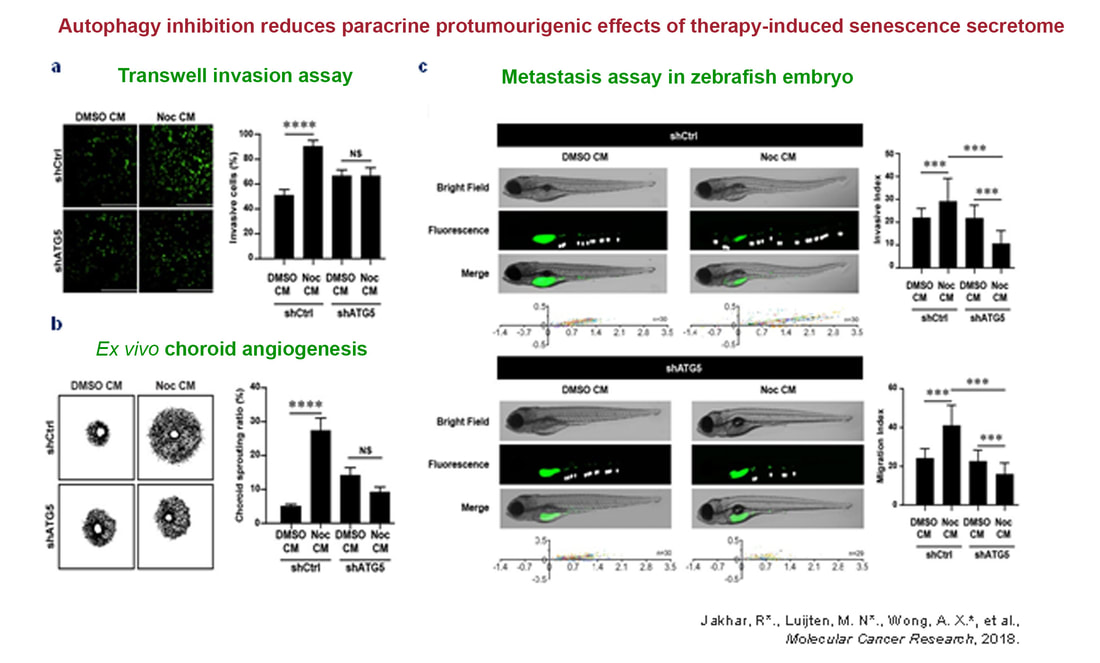
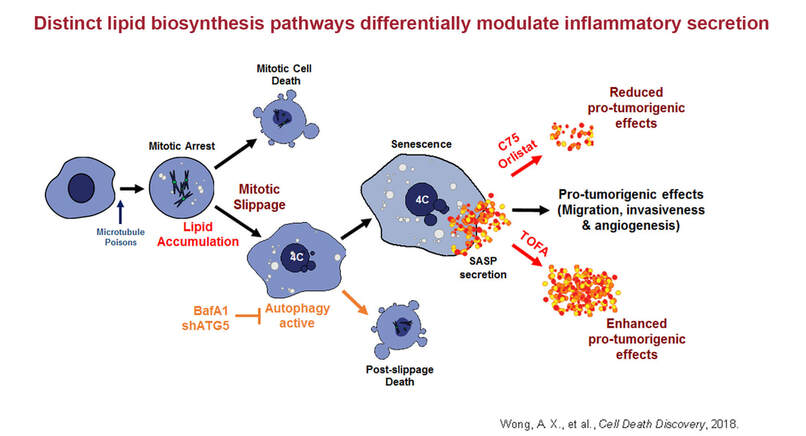
The overarching goal of the lab is to integrate personalised medicine into clinical practice from a chromosomal instability (CIN) perspective. A better understanding of the biology behind cellular response and resistance to chemotherapy is critical for improving outcomes of patients with cancer. We recently described a non-cell autonomous role for CIN that invoked ER stress, autophagy and lipidomic changes culminating in pro-tumorigenic inflammatory secretion. Overcoming therapy resistance requires a thorough understanding of the mechanisms underlying immune evasion by tumours. We are currently dissecting this via time-lapse microscopy, proteomics, RNA-seq, 3D co-culture, single-cell sequencing and immune phenotyping.
The overarching goal of the lab is to integrate personalised medicine into clinical practice from a chromosomal instability (CIN) perspective. A better understanding of the biology behind cellular response and resistance to chemotherapy is critical for improving outcomes of patients with cancer. We recently described a non-cell autonomous role for CIN that invoked ER stress, autophagy and lipidomic changes culminating in pro-tumorigenic inflammatory secretion. Overcoming therapy resistance requires a thorough understanding of the mechanisms underlying immune evasion by tumours. We are currently dissecting this via time-lapse microscopy, proteomics, RNA-seq, 3D co-culture, single-cell sequencing and immune phenotyping.
|
|
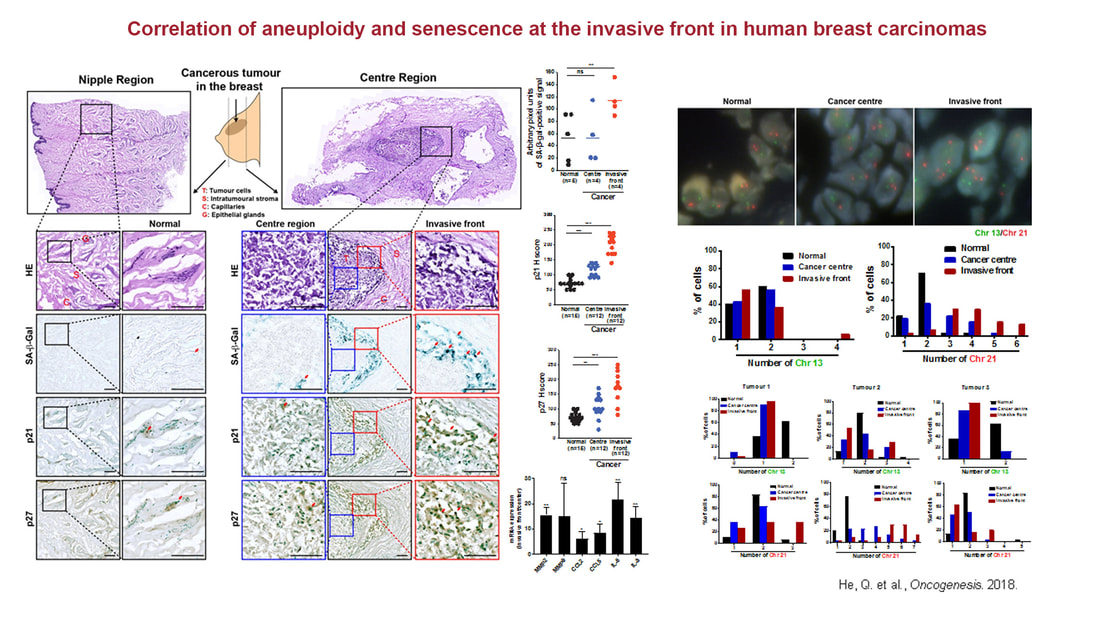
Another focus of research in the lab is studying fundamental cell biological questions in the ageing-cancer nexus. Ageing is the biggest risk factor for cancer. For instance, a large proportion of breast cancers are diagnosed in post-menopausal women (over the age of 50) with mortality rates set to escalate due to our rapidly-ageing population. Additionally, primary glioblastoma, the most aggressive primary brain tumour, typically appears suddenly in older adults. It has been shown that the ageing tumour microenvironment can directly engender a pro-tumourigenic environment over time. We and others have shown non-cell autonomous mechanisms of senescent cells in modulating inflammation via the senescence-associated secretory phenotype (SASP). Ageing is accompanied by accumulative senescence and senescence-associated inflammation. What are the intrinsic processes that initiate SASP and inflammation during aging? How do CIN-associated alterations in the aging stroma drive tumourigenesis? How does cancer and cancer therapy accelerate ageing and ageing-associated diseases? At the NUHS Centre for Healthy Longevity (CHL), we are well-positioned to interrogate these questions as well as explore novel angles in the cancer-aging nexus. It is hoped that these strategies will inform early intervention and treatment strategies in our elderly population.